


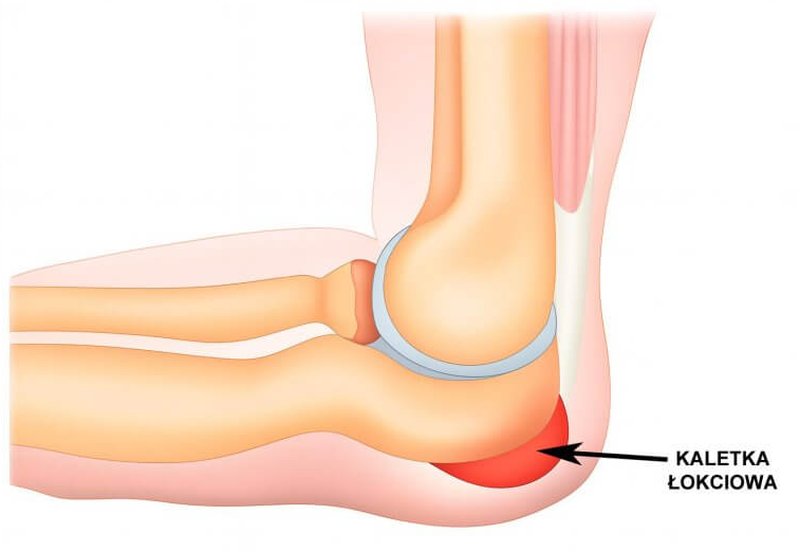
Where is the olecranon bursa located and what is its function?
The olecranon bursa is a small, fluid-filled sac located between the skin and the olecranon process of the ulna—the most prominent part of the elbow. Its main function is to reduce friction and protect soft tissues from mechanical injury, especially during flexion and extension of the elbow joint. It acts like a natural “cushion,” absorbing pressure and allowing smooth movement of the skin over the bone. Thanks to the bursa, everyday activities such as leaning on a desk or supporting oneself with the hands do not cause pain or tissue damage.
What are the causes of olecranon bursitis?
Most common causes:
- Mechanical trauma – repetitive pressure or blows to the elbow area (e.g., prolonged leaning on hard surfaces) may irritate the bursa and cause inflammation.
- Occupational or sports-related overuse – frequent flexion and extension of the elbow, e.g., in athletes, manual workers, or musicians, can lead to microtrauma and inflammation.
- Degenerative changes – exacerbation of degenerative changes in the olecranon process, e.g., fracture of an olecranon osteophyte.
Less common causes:
- Bacterial infections – microorganisms (most commonly Staphylococcus aureus) may enter the bursa through cuts, abrasions, or puncture wounds, leading to purulent bursitis.
- Inflammatory diseases – autoimmune conditions such as rheumatoid arthritis or gout can cause chronic inflammation of bursae, including the olecranon bursa.
- Other factors – poor posture, anatomical abnormalities, and obesity can increase the risk of overloading the elbow joint structures, including the bursa.
Septic vs. aseptic olecranon bursitis
- Aseptic olecranon bursitis is inflammation unrelated to infection—usually caused by trauma, overuse, or inflammatory disease. It presents with swelling and pain without signs of infection.
- Septic bursitis, on the other hand, results from bacterial infection and is often accompanied by skin redness, fever, severe pain, and the presence of pus in the bursa, requiring urgent medical intervention.
What are the symptoms of olecranon bursitis?
- Swelling around the elbow – usually the first noticeable symptom; the bursa fills with fluid and creates a visible protrusion over the olecranon.
- Pain – ranging from dull discomfort to sharp pain, which worsens with pressure or elbow movement.
- Limited mobility – swelling and pain may cause stiffness and difficulty fully extending or flexing the elbow.
- Redness and warmth of the skin – especially in septic bursitis, when the immune system is actively involved.
- Fever and general malaise – systemic symptoms mainly occur with infected bursitis and may indicate the need for urgent treatment.
How is olecranon bursitis diagnosed?
Diagnosis begins with a detailed medical history and physical examination. The physician evaluates the elbow’s appearance and swelling, checks for tenderness, range of motion, and systemic symptoms such as fever.
Bursal fluid aspiration may be performed—its appearance helps distinguish septic from aseptic bursitis, while laboratory analysis determines whether a bacterial infection is present and identifies the pathogen.
Imaging tests are also useful:
Ultrasound (USG) is most commonly used to assess the amount of fluid and inflammatory changes.
X-ray may be done to rule out fractures or bone changes (e.g., olecranon osteophytes).
In chronic or recurrent cases, the doctor may order rheumatologic tests or blood tests (e.g., ESR, CRP, uric acid levels) to exclude systemic diseases such as gout or rheumatoid arthritis.

Treatment of olecranon bursitis
Conservative treatment depends on the cause and severity of symptoms.
For aseptic bursitis, rest, avoiding pressure on the elbow, cold compresses, and anti-inflammatory medications are usually sufficient.
Temporary immobilization with an elastic bandage or brace may be helpful.
Sometimes, aspiration of the bursa is performed to remove excess fluid and relieve pressure, occasionally combined with corticosteroid injection.
If infection is present (septic bursitis):
Treatment also includes oral or intravenous antibiotics, depending on severity.
Regular medical follow-up is essential to assess effectiveness and prevent recurrence or chronicity.
When is surgical removal of the bursa necessary?
Surgical removal of the bursa, known as bursectomy, is considered when conservative treatment fails or when bursitis is recurrent or chronic.
Indications include:
Septic bursitis unresponsive to antibiotics.
Recurrent infections despite treatment.
Large, painful bursae with thickened walls or calcifications causing constant discomfort and limiting mobility.
The goal of bursectomy is to permanently remove the inflamed bursa, which usually restores full function and significantly reduces the risk of recurrence.
How long does treatment last?
The duration of treatment depends on the cause, severity, and chosen therapy.
Mild, aseptic cases – improvement may appear within a few days of conservative treatment, with complete recovery typically in 1–3 weeks.
Septic bursitis – treatment may take several weeks, especially if antibiotics or surgery are required.
Chronic or recurrent cases – treatment may extend over several months, particularly if bursectomy and subsequent rehabilitation are necessary.
Regular medical monitoring allows treatment to be adjusted and shortens recovery time.

