


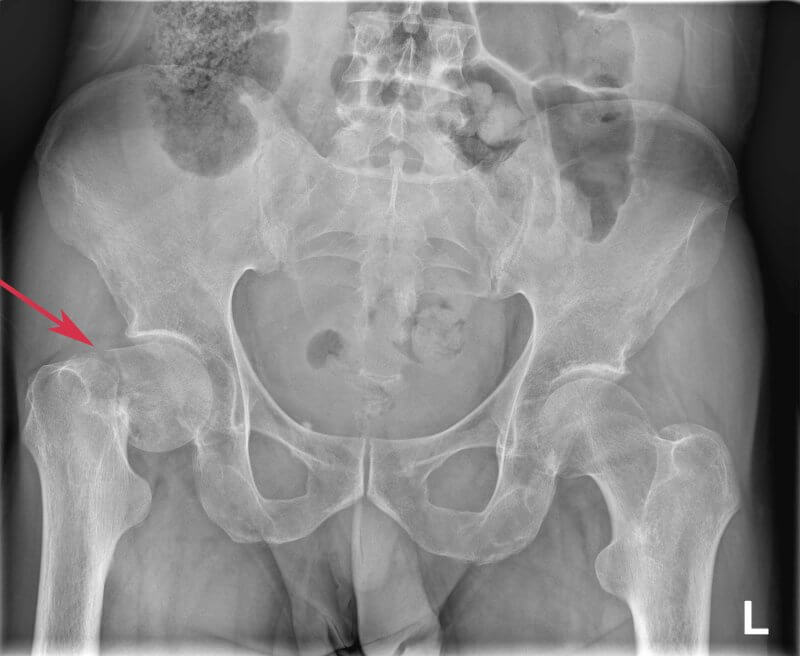
Location of the femoral neck fracture
The hip joint is a ball-and-socket joint formed by the acetabulum of the pelvis and the head of the femur (caput femoris). It is surrounded by a joint capsule and stabilized by strong ligaments. The femoral neck, the site of the fracture, connects the head of the femur to the shaft and lies within the joint capsule—hence it is classified as an intracapsular structure. Its blood supply comes mainly from the circumflex femoral arteries, which makes this area particularly vulnerable to ischemia in the event of injury. A fracture of the femoral neck can disrupt the blood flow to the femoral head, leading to avascular necrosis (osteonecrosis). Due to its anatomical location and limited blood supply, fractures in this region are difficult to treat and most often require surgical intervention.
Causes of a femoral neck fracture
A femoral neck fracture most commonly results from a low-energy injury, such as a fall from standing height, particularly in elderly patients with osteoporosis. In younger patients, it may result from high-energy trauma, such as a motor vehicle accident or a fall from a significant height. In some cases, the fracture may be pathological, caused by weakening of the bone structure due to conditions such as cancer, osteoporosis, or chronic osteomyelitis.
Risk factors for femoral neck fracture
- Advanced age (especially over 65 years)
- Osteoporosis
- Female sex (due to lower bone mass and hormonal changes after menopause)
- Impaired balance and muscle weakness (e.g., sarcopenia)
- Neurological disorders (e.g., Parkinson’s disease, dementia)
- Visual impairment
- Low body weight and malnutrition
- Use of medications increasing fall risk (e.g., benzodiazepines, antihypertensive drugs)
- Previous fall or osteoporotic fracture
- Lack of physical activity
- Alcohol abuse or smoking
- Chronic diseases (e.g., diabetes, rheumatoid arthritis)

Mechanisms of injury
Femoral neck fractures can be divided into two main groups depending on the energy of the injury:
- Low-energy injuries (most common in the elderly): Typically occur from a fall from standing height, often while walking or changing position. In people with osteoporosis, even minimal force (such as tripping over a doorstep) can cause a fracture.
- High-energy injuries (more common in younger patients): Result from motor vehicle accidents, falls from great heights, or sports injuries. These fractures are often complex, with significant displacement and associated soft tissue damage.
Types of femoral neck fractures
The most common classification systems include:
Garden classification (most commonly used): Determines the degree of displacement, which is critical for treatment planning:
I – Incomplete or valgus impacted fracture, without displacement.
II – Complete fracture, without displacement.
III – Complete fracture with partial displacement.
IV – Complete displacement with no contact between fracture fragments; highest risk of femoral head necrosis.
Pauwels classification (based on the angle of the fracture line to the horizontal): Used to assess the forces acting on the fracture and the risk of instability:
Type I – angle <30° (low risk of displacement)
Type II – angle 30–50°
Type III – angle >50° (high risk of displacement and conservative treatment failure)
Anatomical classification:
Subcapital fracture – just below the femoral head
Transcervical fracture – through the middle of the neck
Basicervical fracture – at the base of the neck, closer to the trochanters
Symptoms of a femoral neck fracture
Patients typically experience sudden, severe pain in the groin or hip following injury, which may radiate to the thigh or knee, especially with movement. They are unable to bear weight on the affected limb, which appears shortened and externally rotated when lying down—due to muscle action. Swelling and tenderness in the groin or hip region may be present but are often moderate, as the fracture is intracapsular. There is marked limitation or complete loss of hip joint mobility, and passive internal rotation is especially painful. Some patients support the injured leg with their hands when attempting to change position, a phenomenon known as the “tripod sign.”
Incidence of femoral neck fractures
Femoral neck fractures are a very common and serious health issue, especially in aging populations. Worldwide, an estimated 1.6 million cases occur each year, and this number is projected to rise to 4.5–6.3 million by 2050, mainly due to population aging (source: International Osteoporosis Foundation). In Poland, over 30,000 proximal femur fractures are reported annually, most of which are femoral neck fractures (data from the National Health Fund and the National Osteoporosis Registry).
Diagnosis of femoral neck fractures
Diagnosis aims to confirm the fracture, assess its type and displacement, and plan treatment. It typically begins with a thorough medical history and physical examination. Patients usually report severe groin or hip pain, difficulty moving, and a shortened, externally rotated limb. These signs already suggest the diagnosis. Confirmation is obtained with pelvic and hip X-rays, which reveal the fracture and any displacement. In cases where the fracture is not visible on X-ray but symptoms persist, more precise imaging is used—such as computed tomography (CT) or, in some cases, magnetic resonance imaging (MRI). These methods allow for fast and accurate diagnosis, which is crucial for timely treatment and preventing complications.
Treatment options for femoral neck fractures
This is a serious injury requiring prompt, tailored treatment. The choice of method depends on whether the fracture is displaced, the patient’s age, general health, and pre-injury functional level. Early treatment increases the likelihood of recovery and reduces complication risk.
Conservative treatment – reserved for rare cases in very elderly, immobile patients with multiple comorbidities, or for very stable, non-displaced fractures. It involves immobilization of the limb and gradual rehabilitation. However, it carries a high risk of bedsores, pneumonia, and venous thromboembolism, and nonunion or malunion may occur, often necessitating later surgery.
Surgical treatment – the gold standard for most patients. Surgery allows early mobilization and reduces the complications of prolonged bed rest. Options include:
Osteosynthesis – internal fixation with screws or plates, used in stable, non-displaced fractures, most often in younger or active older patients. This method preserves the natural hip joint but requires adequate blood supply to the femoral head.
Arthroplasty – joint replacement, used for more complex, displaced fractures. This may be hemiarthroplasty (replacement of the femoral head only, preserving the natural acetabulum) in less active elderly patients, or total hip arthroplasty (THA) (replacement of both the femoral head and acetabulum) in active older patients, especially with pre-existing osteoarthritis. Arthroplasty allows rapid mobilization, often within days of surgery.
Timing of surgery
Surgery should be performed as soon as possible—preferably within 24–48 hours of hospital admission—to reduce the risk of complications and improve the chances of regaining independence.

Postoperative rehabilitation
Rehabilitation starts within the first days after surgery. Early mobilization helps prevent serious complications such as pneumonia, thrombosis, and muscle weakness. Patients are encouraged to stand and start exercises—initially with a walker or crutches—under the supervision of a physiotherapist. Therapy includes gait training, range-of-motion and strengthening exercises, balance training, and increasing independence in daily activities. The rehabilitation period may last from several weeks to months, with ongoing physiotherapy often required for older adults. Prevention of further fractures is essential and may include osteoporosis management with calcium and vitamin D supplementation, anti-osteoporotic medications, and lifestyle modifications.
Prognosis
Outcome depends on age, pre-injury health, time to surgery, type of operation, and quality of rehabilitation. Among patients over 80 years old, 20–30% die within one year of the fracture, mainly due to systemic complications. Around 50% never regain full independence, and some require permanent care. In younger or previously active patients, full recovery is often achievable.
Prevention
Femoral neck fractures in the elderly are highly dangerous, carrying a significant risk of permanent disability, loss of independence, and death within 12 months after injury. To reduce risk, measures include osteoporosis prevention (calcium and vitamin D supplementation, pharmacologic therapy), age-appropriate physical activity, avoiding medications that cause excessive blood pressure drops or impair balance, and ensuring a safe home environment by removing tripping hazards, installing handrails, and improving lighting. Regular check-ups and support from family or caregivers are also crucial in preventing falls and injuries.






