


Causes of Femoral Neuralgia
Femoral neuralgia is classified as a type of radiculopathy, characterized by irritation or compression of the nerve roots (typically L2–L4) that form the femoral nerve and innervate the anterior thigh and part of the knee. In most cases, the primary cause is a bulging or herniated intervertebral disc, commonly at the L2–L4 level, accompanied by degenerative changes such as osteophytes, ligament thickening, or spinal canal stenosis.
Mechanical and structural factors that may lead to nerve root compression include improper tension in the iliopsoas muscle, spinal injuries, inflammatory conditions, or trauma involving the pelvis or abdominal cavity, which may disrupt the space available for nerve roots.
Metabolic and systemic conditions, such as diabetes, can also predispose to nerve damage by causing neuropathy or microcirculatory changes within the nerve, increasing its susceptibility to compression. Lifestyle and biomechanical factors are also significant—prolonged sitting, physical overload, obesity, sedentary lifestyle, or even intense workouts can strain spinal structures and paraspinal muscles. Additionally, although rare, the etiology may be idiopathic, with no identifiable cause.
Symptoms of Femoral Neuralgia
1. Pain and Sensory Disturbances
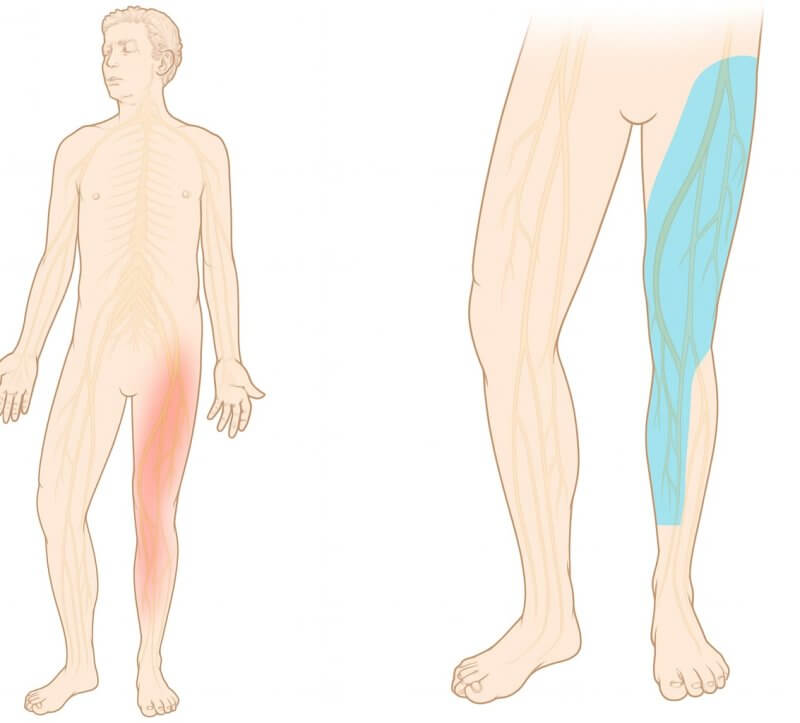
- Pain characteristics: Usually sharp, shooting, burning, or electric-like. Patients often describe it as a “current” running through the front of the thigh.
- Pain location: Typically begins in the lumbosacral region and radiates to the anterior thigh, knee, inner calf, and sometimes the foot.
2. Sensory Changes (Paresthesia)
- Sensory symptoms: Numbness, tingling, burning, or stabbing sensations—mainly in the anterior and medial thigh, sometimes involving the knee or calf.
- Decreased sensation: Reduced tactile perception in areas innervated by the femoral nerve—mainly the anterior and medial thigh and part of the calf.
3. Motor Dysfunction and Muscle Weakness
- Paresis or paralysis: Weakness in knee extension and difficulty with hip flexion due to impaired innervation of the quadriceps and iliopsoas muscles.
- Gait impairment: Knee instability, with a feeling of the knee “giving way” or “slipping” during walking.
- Muscle atrophy: In severe or prolonged cases, visible atrophy of the quadriceps muscle.
4. Reflex and Muscle Tone Abnormalities
- Absent knee-jerk reflex: Diminished or absent patellar reflex.
- Increased paraspinal muscle tension: Often seen as a protective response to pain and nerve injury.
- Postural deviation: Patients may adopt an asymmetrical posture to avoid pain.
5. Mackiewicz Sign
- Specific diagnostic test: Pain in the anterior thigh triggered by passive knee flexion while the patient lies prone or on their side.
6. Red Flag Symptoms (in severe cases)
- Muscle paralysis: Complete loss of motor function in the lower limb.
- Severe sensory loss: Involving large areas beyond the affected limb—requires urgent evaluation.
- Bladder or bowel dysfunction: Loss of control over urination or defecation may indicate serious neurological damage and demands immediate medical attention.
Diagnosis of Femoral Neuralgia
Diagnosis primarily relies on a detailed medical history and thorough neurological and orthopedic examination. The physician assesses the pain's location and nature, evaluates muscle strength, range of motion, patellar reflex, and looks for characteristic signs such as Mackiewicz’s sign (pain with passive knee flexion in a lying position).
To confirm the diagnosis and determine the underlying cause, imaging studies are conducted—most commonly magnetic resonance imaging (MRI), and less frequently computed tomography (CT) or X-rays, which help visualize spinal changes and nerve root compression. Additional testing may include electrophysiological studies, such as electromyography (EMG), to assess femoral nerve function.
The purpose of the diagnostic process is not only to confirm femoral neuralgia but also to rule out other conditions with similar symptoms.
Treatment of Femoral Neuralgia
Treatment is multifaceted and includes both conservative methods and, in more severe cases, surgical intervention.
In the acute phase, therapy focuses on pharmacological management:
- Pain relievers and anti-inflammatory drugs (NSAIDs)
- Muscle relaxants
- Short-acting steroid injections near the nerve roots in cases of severe pain
Rehabilitation plays a crucial role—individually tailored stretching and strengthening exercises for abdominal and back muscles help offload the spine and reduce pressure on the femoral nerve.
Physiotherapy may include:
- Laser therapy
- Cryotherapy
- Electrotherapy
These modalities help reduce inflammation and muscle tension.
In chronic cases or when conservative treatments fail, surgical options may be considered—most commonly discectomy (removal of the herniated disc) or spinal decompression.
An essential aspect of treatment is addressing risk factors such as excess weight and physical inactivity to lower the chance of recurrence.
Prevention of Femoral Neuralgia
Prevention focuses on maintaining spinal and muscular health and minimizing risk factors for recurrence.
Key strategies include:
- Regular physical activity, especially exercises that strengthen the abdominal, back, and gluteal muscles, which stabilize the lumbar spine and reduce mechanical strain
- Proper ergonomics in work and daily life—avoiding prolonged sitting, ensuring proper back support, and using correct lifting techniques (with bent knees, not straight legs)
- Maintaining a healthy body weight, as obesity increases spinal load
- Taking regular breaks during sedentary work, stretching the iliopsoas muscles, and avoiding sudden or jerky movements
- These measures not only help prevent femoral neuralgia but also support the overall health of the spine and musculoskeletal system.

